Hi Kel,
Been busy at work, so not a lot of time to post.
Regarding E2, the normal guy on TRT should not fear E2, even if it becomes slightly out of range. E2 is made from T, so when T goes up so will the rate of conversion to E2. It's a simple mass-action enzymatic conversion. The more T you feed the aromatase enzyme, the more E2 you will get. The simple solution for guys on TRT is to move to lower and more frequent dosing of T so that your peak and nadir levels of T always stay within or close to the "normal" range. E2 will follow.
The problem is when guys just don't get this and approach TRT with a 'more is better' approach, or use old school protocols of once weekly or (God forbid) once ever 2 week protocols. With these old school protocols still prescribed and promoted by dinosaur doc, comes huge spikes in T at the beginning of the injection cycle in order to keep nadir levels within range at the end of the injection cycle. Therein comes the huge spike in E2 at the beginning of the cycle which takes some time for the body to clear, and then you do it all over again but this time building on the uncleared levels of E2 from the prior injection cycles. It's a hormonal roller coaster ride to hell!
Guys are paranoid of E2 because of bro talk in the locker room. Bodybuilders sometimes have problems with gynecomastia and they blame it on E2. Which has some basis in reality, but the real truth is that they are often stacking many anabolic hormones on top of each other and at the base of these stacks are way higher doses of T than we use in TRT. The huge doses in T (e.g., 300-500 mg/week), cause spikes in E2, which of and by itself is not horribly bad, but many of the other synthetic anabolic agents they stack with the T (e.g., nandrolone) also have affinity to the progesterone (P4) receptors in the body. High E2 + P4 is a recipe for gynecomastia. This is what happens in the 3rd trimester of pregnancy when the placenta takes over hormone production in women. It pumps out huge amounts of both of these hormones in order to prepare the breast tissue for lactation, so there is rapid development of the mammary glands. Throw in high levels of prolactin (or in the case of pregnancy placental lactogen which has prolactin-like activity) and you begin to lactate. Many of the synthetic anabolics also have a propensity to bump up prolactin levels. I've seen videos on the internet of bodybuilders lactating. It's not pretty!
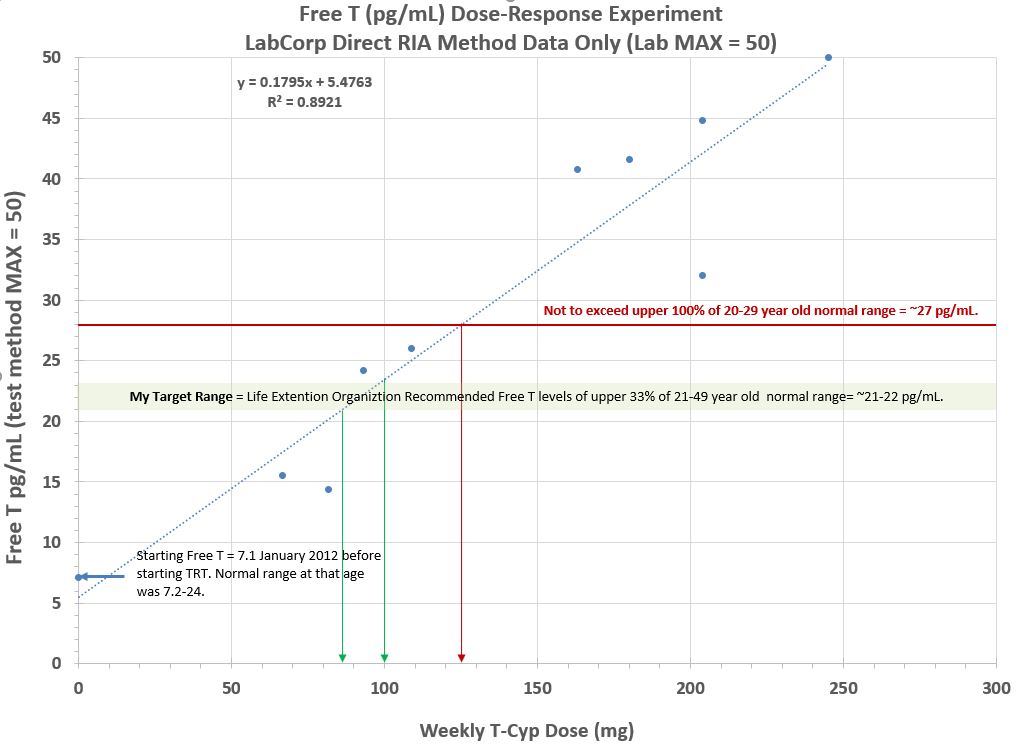
Coming back to nandrolone, it's new to me Kel. I've only been experimenting with it for about 2+ weeks to see if I can get some relief from my elbow injury from 2 years ago. It seems to be working well. The moderate anabolic boost is an added perk too, but not my primary motivation (I've got more than enough muscle mass from 20+ years of weight lifting). I've been experimenting with various doses of T over the past year too in order to optimize my Free T without having to use synthetic anabolics (e.g., stanozolole or Oxandrolone (Anavar))
to suppress my high SHBG. I've selltled on 125 to 140 mg/week E3D protocol as my optimal protocol. This keeps my E2 from going way out of range and bring my Free T within the Target range.
Can't remember if I've posted the graph of my T range-finding experiment in this forum. Here is is:






 Reply With Quote
Reply With Quote


