Didn't forget I just haven't gathered any info on it until now. Going to scrounge up what info I have and see what I can do. Thanks for looking out bro.Originally Posted by stevey_6t9



 AR's Think Tank
AR's Think Tank

Didn't forget I just haven't gathered any info on it until now. Going to scrounge up what info I have and see what I can do. Thanks for looking out bro.
AR's Think Tank
The Male Hormone Panel
The aging process is inevitable. However, restoring lost male vitality is within reach. The hormones involved in this restoration can now be collectively measured in one salivary panel using the Regular or Expanded Male Hormone Panels (MHP and eMHP). The problems that concern men that most can be grouped into 3 categories:
Vigor:
- loss of sense of well being
- difficulty concentrating
- depression
- irritability and nervousness
- alternation in behavioral patterns
- change in sleep habits/insomnia
Vitality
- decrease in hair density
- reduction in masculinity
- decrease in muscle mass and strength
Virility
decline in sexual function and interest, diminished libido and erictile dysfunction (ED)
- decrease in bone mass (osteoporosis)
Andropause
At around puberty, the important male hormone, testosterone, reaches adult levels. For a long time it was believed that men maintain adequate levels of testosterone throughout life. Many men in their fifties or older however, experience a progressive decline in their energy, vitality, sexual performance and mental capacity. This decline has been labeled "Andropause." The causes of andropause are believed to be a reduction in testosterone and other androgens. The testicles show a progressive annual drop of 1-1.5% in testoterone output after age 30. Furthermore, as men age, a 1-2% in both Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH) has been documented. The clinical manifestations of andropause usually lag ten to twenty years behind the onset of hormone decline. Statistically, andropause effects at least 40% of men ages 55-65, and up to 80% of those aged 65 years or more.
Knowing the levels of the 6-8 hormones measured in the Male Hormone Panels helps you formulate an effective plan to relieve andropausal symptoms.
Regular Male Hormonal Panel (MHP)
Several years ago, Diagnos-Techs, Inc. introduced the first salivary Male Hormonal Panel which evaluates the androgen pathway by measuring the free fractions of the hormones shown below.
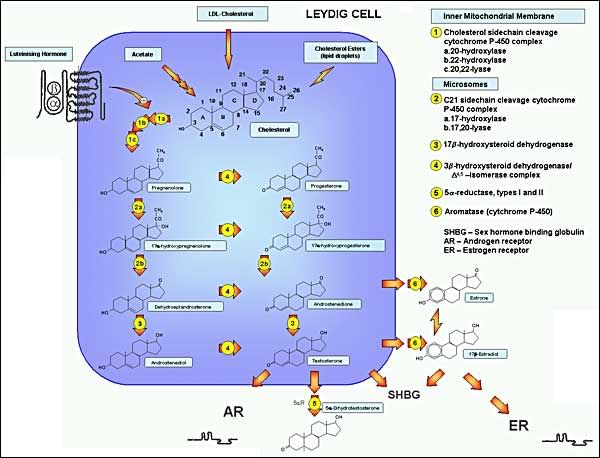
FIGURE 1. Pathways of testosterone biosynthesis and action. In men, testosterone biosynthesis occurs almost exclusively in mature Leydig cells by the enzymatic sequences illustrated. Cholesterol originates predominantly by de novo synthesis pathway from acetyl‑CoA with luteinizing hormone regulating the rate‑limiting step, the conversion of cholesterol to pregnenolone within mitochondria, while remaining enzymatic steps occur in smooth endoplasmic reticulum. The ï„5 and ï„4 steroidal pathways are on the left and right, respectively. Testosterone and its androgenic metabolite, dihydrotestosterone, exert biological effects directly through binding to the androgen receptor and indirectly through aromatization of testosterone to estradiol, which allows action via binding to the ER. The androgen and ERs are members of the steroid nuclear receptor superfamily with highly homologous structure differing mostly in the C-terminal ligand binding domain. The LH receptor has the structure of a G-protein linked receptor with its characteristic seven transmembrane spanning helical regions and a large extracellular domain which binds the LH molecule which is a dimeric glycoprotein hormone consisting of an α subunit common to other pituitary glycoprotein hormones and a β subunit specific to LH. Most sex steroids bind to sex hormone binding globulin (SHBG) which binds tightly and carries the majority of testosterone in the bloodstream.
1. Progesterone is a precursor to all androgens and is a physiologic modulator of DHT production
2. DHEA & DHEA-S, the main adrenal androgens are the precursors to both testerone and estradiol, and the limiting factor in their production especially under stress.
3. Androstenedione, another adrenal androgen and precursor to estrone is freely inter-convertible with testosterone.
4. Estrone is the major estrogen in mend and is the product of peripheral aromatization of androstenedione in fat and muscle tissue.
5 & 6 Testosterone, the dominant testicular androgen, is the precursor to 5-dihydrotestosterone (DHT). The androgenic effect in various tissues is not exerted by testosterone buy by the locally produced DHT.
Expanded male hormone Panel (eMHP)
This panel includes all the 6 tests in the regular MHP, plus FSH and LH. Sallivary quantitation of FSH and LH is a technological breakthrough that seperates Diagnos-Techs from the crowd of copycat laboratores. Testosterone and sperm production in males are the equivalent of estrogen and ovulation in females. The pituitary neurohormones, FSH, and LH, stimulate and regulate sperm atogenesis and testosterone production respectively.
- Early detection of an increase in FSH and LH levels is indicative of a progressive decline in male sexuality and functionality. The clinical utility of the Male Hormone Panel is shown in the:
- Measuring of baseline hormones
- Diagnosing andropause and hypogonadism
- Therapeutic monitoring of HRT
- Balancing of hormones
- Investigating of prostate hypertrophy, thinning of hair and hirsutism
- Evaluating of low-libido in both sexes
Beneficial Effects
Following the use of MHP/eMHP, treatment plans using hormones to replace the balance of endogenous production usually produce several positive effects:
- Increase of fitness and sense of well-being
- Decrease of body fat and increase in lean body mass
- Resolution of hormone dependent libido problems
- Prevention of hair thinning
- Increase of hematocrit and RBC counts
- Mitigation of esteoporosis and stimulation of bone formation
- Decrease in total cholesterol, increase in HDL
*Note* Unmonitored male HRT may account for increased incidence of prostatic complications, liver cancer, and accelerated atherosclerosis.
-Diagnos-Techs. INC.
David J Handelsman MB BS, FRACP, PhD Director, ANZAC Research Institute & Department of Andrology, Concord Hospital, Professor of Reproductive Endocrinology & Andrology, University of Sydney,Sydney, NSW 2139, Australia
There are currently 1 users browsing this thread. (0 members and 1 guests)
 Posting Permissions
Posting Permissions

 Reply With Quote
Reply With Quote