


Results 1 to 37 of 37
 5Likes
5Likes
 LinkBack URL
LinkBack URL About LinkBacks
About LinkBacks-
04-27-2019, 06:04 AM #1

 Junior Member
Junior Member

- Join Date
- Jun 2018
- Posts
- 114
Trt bloodwork - Low dose T, very high total T, normal-low SHBG.
I just did my bloodwork after staying consistent with my new trt protocol (70mg per week, dosed EOD).
Total T: 13.6ng/ml (2.8 - 8.0)
Estradiol: 88.5pg/ml (11.3 - 43.2)
SHBG: 16.03nmol/l (11.4 - 52.3)
Free T: still have to wait a week. I suppose super high given the shbg level? I will update it when I have it.
DHT: I wanted to check because I had some little hair loss, but the lab didn't do it
I have been only a month on it (after a little break), I expect it could build up to even higher levels with time. I always felt like I have an unusual response to exogenous test. It feels like I'm injecting 2x the stuff I'm actually injecting
I feel the high E levels though. Libido is gone compared to what it used to be, morning wood is gone, I don't feel as much energy as in the earlier days and my muscles, my torso, everything looks like water balloons. Fortunately I have some room to lower the dosages. I think I will try to go as low as 70% of what I'm injecting now, I will just need to check what Free T will be. Can I use insulin syringes? Because I'm already injecting 0.1ml, I will have to go even lower.
By the way, if I have already low shbg, are there any additional benefits with running 5000iu D3 (along with magnseium and K2)?
-
04-27-2019, 01:38 PM #2
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
I would double check the label on the T and your dose calculations. Make sure they are correct. Your prior dose of 40mg E3D is a fairly typical starting dose and should not be sending your T levels so high. On the other hand, you are on the lower end of the SHBG range, so that might account for the rapid spikes in T and conversion to DHT and subsequent hair loss. Originally Posted by mac34
Originally Posted by mac34

Your E levels are on the high side and should come down by lowering the T dose. I suspect the low SHBG has a lot to do with the high E levels too. T converts rapidly to E2 without SHBG to buffer it.
Since you already have low SHBG, I would not add in in D3. That would just lower it more. I have no idea of the effect of mg or K2 on SHBG.
Guys with low SHBG tend to do better with small daily injections of T. many do it subcutaneously. When you drop the volume down that low for daily injections, the use of an insulin syringe is best both for comfort and for accurate measurement. I would consider using a 0.5 mL 28G syringe with a 1/2 inch needle. I use these to inject 0.2 to 0.25 mL of my T on an E3D protocol and it works very well for me.
-
04-27-2019, 03:13 PM #3
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Thanks for your answer. That makes sense. I remember I felt my first gear injection within hours. I don't think it was placebo, happened 2 times and with that E3D, E4D dosing I always had the pump on the day on, day after, and all gradually dropped, until on day 3 I didn't feel anything. I was almost wondering if it wasn't test propionate . Originally Posted by Youthful55guy
But that's why I do EOD 20mg for a month now, and that dosing is what made these results. So it's even more crazy, I inject 0.1ml, lowest of the scale, E2D and get what seems to be 30-70% more than the max total T range (depending on the range). I also did a test in a different lab 1.5week prior. T level was 8.4, but that was 5 shots earlier, it might still be building up.
I'm pretty sure calculations are right. Gear is 200mg/ml. I inject 0.1ml, so it's 20mg EOD = 70mg per week I always used the same ugl. My friend is also using it, and it works like a normal gear for him.
Perhaps I should consider the daily injections. But then I assume I would be injecting 0.02-0.04ml . Maybe I would switch to subq, but if not, can I use a slin syringe with a longer needle for intramuscular injections?
-
04-27-2019, 03:37 PM #4
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
I would drop down to 0.05 mL daily dosing with a 0.5 mL 28G insulin syringe with a 1/2 inch needle. This will allow you to go either IM or subcutaneous, whichever you find works best for you. I tend to bruise easily with subcutaneous, so I inject IM into the upper outer Quad and I outlined in the "Best Practices" sticky (see diagram). You can also use deltoids with that small needle size if it is easier. This protocol will deliver 70mg per week but very small peeks and valleys in the dosing. This more constant dosing schedule should work better with your low SHBG and give you more consistent T values that are always in range. Originally Posted by mac34
-
04-27-2019, 10:20 PM #5
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
So do you think that the day after injection my T levels are much higher than the day of injection? I inject in the mornings, and do bloodwork in the morning the next day. Originally Posted by Youthful55guy
I think one way to find out would be to do the test again, and the day after, skip the injection and do another test and compare what is a 1 day drop.
But I don't think that T metabolizes that fast in me. I think it is normal. With 40mg every 3-4 days, final time I made a mistake and injected 80mg instead of 40mg. I didn't do any injections after (I lost my last vial and had to wait). I felt on for 2 more weeks (and even more on, as E was dropping faster than T). After 2-3 weeks of that last injection T readings showed 5.6. So while I mentioned it felt like propionate , because of the sudden kick, it still "sticks" over time and I'm not sure if I would benefit that much from every day injections, or if it would make my T drop in range.
Also the kick I experienced might as well been due to T/E ratio.
-
04-28-2019, 11:34 AM #6
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
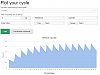
Here's a web site you might find helpful in answering T levels from various T esters and/or using various injection protocols: SteroidGraph - Graph your cycle
Keep in mind that the software calculates the amount of T released from the T ester per day (i.e., not T levels in your blood). T levels in your blood will be highly influences by SHBG. Guys with high SHBG (like me) will show higher Total T levels because SHBG protects T from liver metabolism BUT we will also show lower levels of Free T (the stuff we really need to feel normal) because most of it is tightly bound into the SHBG protein and ever so slowly released.
Guys with low SHBG (like you) will show the opposite. You will have lower Total T because it's being burned off rapidly in the liver and higher Free T for a short period of time after (what's left of the ester ) releases its T. it's a complicated interaction between the ester release and metabolism. It also shows why the Total T test is a waste of money and gives misinformation for guys who do not have "normal" SHBG levels.
When interpreting these graphs, you can use the general guideline that the normal health adult male produces about 7 mg T per day. This is a good figure to interpret the T released from the ester because our endogenous system is shut down while on TRT. here's a couple of graphs you might find interesting. You can customize the graphs to your own situation.
40 mg T-Cyp E3D (my regular protocol low dose)
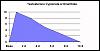
50 mg T-Cyp E3D (my regular protocol high dose)
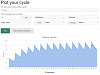
10 mg T-Cyp (0.05 mL) daily (close to what you are considering)

-
04-28-2019, 12:55 PM #7
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
That's a nice tool. Thanks for the graphs. It seems like there isn't a huge difference between every day and every other day, but e3d highs and lows are noticeable - the graphs seem to match what I felt.
The thing is, if I have low SHBG, my total T should be lower, right? So why does it get out of range, despite the low doses, and low SHBG? I would understand if I had high total T with high SHBG, but I have unusually high total T, with low SHBG. I just wonder what the Free T will show - I will get the results in a week.Last edited by mac34; 04-28-2019 at 12:59 PM.
-
04-28-2019, 07:06 PM #8
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
It's because of when you do your lab draws. You stated earlier that you pull blood the morning after your injection. See the graph below. That's when you T-levels are the highest. They release much of their T within the first 24 hours and then slowly deplete their T release over about 8-10 days. However, in your case, you have little SHBG to absorb the T and protect it from liver metabolism, so the released T is rapidly removed from your body. Originally Posted by mac34
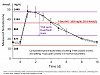
Most TRT docs have you test immediately before your next injection so that you catch the nadir, not the peek levels.
-
04-30-2019, 08:55 AM #9
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I have tested it and the difference between 24h vs. 48h in EOD cycle was 1.3ng/ml. I have also noted down some more recent details regarding bloodwork and injections: Originally Posted by Youthful55guy
There are a few remarks I can make:Code:2019.04.16 * Lab-A bloods: T: 8.40, E: 79.05 (24h after injection) * This was also a time where I felt on 2019.04.26 * Lab-B bloods: 13.6 T, E: 88.5 (24h after injection) 2019.04.27 * Feeling a bit off. Pretty sure it was the increased estradiol * This day I didn't do the injection, broke EOD cycle 2019.04.28 * Injection after 72h. Rear delt shot could go a bit wrong. 2019.04.29 * Lab-A bloods: T: 6.63, E: 53.60 (24h after injection) 2019.04.30 * Lab-A bloods: T: 5.36, E: 62.60 (48h after injection, before next injectiion)
* Lab-B could have been way off with that high reading
* Breaking injection cycle (injecting after 72h instead of 48h) could have lowered the levels I got on 2019.04.29. Even with the same lab, 2 weeks ago I had 8.40 T, yesterday it was 6.63. Both were done 24h after injection.
* 48h after injection showed 5.36. This is just 1.3ng/ml down from the day before (20% less)
Do you think I should still try every day injections? Thank you for all your help
Last edited by mac34; 04-30-2019 at 08:59 AM.
-
05-02-2019, 03:16 AM #10
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I'm going to give it a try with ED injections, use insulin syringes for measuring and inject IM. Ideally I would find a slin syringe with swappable needle.
In case I do not, I would go with 28G slin syringe or whatever is the biggest size I could find at a pharmacy. In that case, would it be fine to draw the oil with a regular syringe, take the plunge out of the slin needle and shoot the oil to the slin needle? I guess there's no other way is it? Because I wouldn't want to use the same slin needle for drawing and injecting.
Or maybe the other way around. Try to draw the liquid with 28G slin needle, measure it, take the plunge out of a normal syringe and shoot all the liquid into the normal syringe.
What do you think?
-
05-08-2019, 12:20 AM #11
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I decided to halve the dose and inject 0.05ml every day. After a few days I noticed my scalp itches all over and hair falls again. It didn't make sense, so I compared the actual volume of using a normal 2ml syringe with 0.10ml precision, and an insulin syringe with 0.05ml precision (by shooting the contents into a 40iu slin syringe). It turns out I used to inject more like 0.06-0.07ml EOD, rather than 0.10ml EOD (equivelent to 40-50mg a week) . Since I switched to the needles with 0.05ml precision and started every day injectons, I have been injecting a comparable dose, every day rather than eod, which probably increased my total intake about 30-40%, hence the hair loss. Originally Posted by mac34
I'm still on the lookout for 40iu slin syringes with replaceable needles. I figure I will have to inject 0.03ml every day, or maybe even less.
I also got the Free T readings, not sure what it was, but it was also above the range.Last edited by mac34; 05-08-2019 at 12:26 AM.
-
05-09-2019, 11:28 AM #12
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
Just a thought. We know from several medical publications that thyroid hormone treatment will increase SHBG. My personal experience and labs corroborate this too. Have you considered adding in desiccated thyroid tables (like Armour Thyroid) to your protocol. if you do, my suggestion is to start at 15mg per day and SLOWLY raise the dose by 15 mg every 2-4 weeks, giving your body time to adjust to the higher doses. I would then redo SHBG labs after 4 weeks at 60mg per day and see how you are doing.
-
05-09-2019, 01:51 PM #13
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Interesting info. I would rather have it where it is and hope the daily injections will fix it. Once I have my TRT perfected, I will consider coming off and trying a PCT, and see where would I be naturally. Low SHBG would come handy then. Originally Posted by Youthful55guy
I found the perfect 1ml high precision syringes with swappable needles. Ordered 100s of them from a pharmacy online Now I will be confident that every time I inject the same dose. I hope the lowered doses every day will bring the estradiol down. If not, I will try the d-something, I forgot what was the name.
By the way, I had a thought that the highly anabolic effects I experienced from 30-40mg twice a week were due to this fast metabolism. E.g. there's the peak where it's almost like being on cycle, muscle grows, then even if the T is lower, I'm still anabolic and won't lose the gains, and then another peak, muscle grows, and so on. I was bigger without going to the gym than now when I go to the gym. But that wasn't proper TRT and that hormone rollercoaster wasn't good for the wellbeing.
-
05-13-2019, 01:33 AM #14
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I don't want to post another thread, I have a quick question. Can I do testosterone /estradiol bloodwork at like 1pm, after eating? Does it matter whether I eat or not for the results of these 2?
-
05-13-2019, 05:26 AM #15
Productive Member
- Join Date
- May 2018
- Posts
- 1,886
It does not matter if you are fasted or not Originally Posted by mac34
Sent from my LG-LS993 using Tapatalk
-
05-13-2019, 05:35 AM #16
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
Fasting doesn't matter as mentioned above. But you should be consistent in bloodwork. Originally Posted by mac34
For example, Can't accurately compare bloodwork results if one day you test Monday at 8am and next time is Wednesday 1pm and the next time is Monday after a hard leg workout etc.
Gotta pick a specific time and day of the week and do it before training with no alcohol 25 hours prior.I no longer check my inbox. If you PM me I will not reply.
-
05-13-2019, 08:22 AM #17
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
Ditto on both of the above comments and I'd add do not take large doses of B vitamins containing Biotin for 4 days before your lab draw. Large doses of Biotin, such as 10-15mg (333-fold greater than the dietary recommendation) can interfere with the assay. I believe it artificially inflates your T values, but need to research that more. But I do know that it interferes with many RIA based hormone assays.
-
05-27-2019, 11:49 PM #18
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Thanks for your answers. I haven't got to do the bloodwork yet. I'm abroad and it's not that convinient as when I was in my hometown. Though I can tell that 3 weeks of microdosing did nothing. I could still wonder if I'm not taking too much (about 6mg per day). Last time I felt really good libido was 3 weeks ago when I started this - I made a 2 day break from injections. Must have been due to E2 lowering, it just makes such a huge difference to me.
Now the only thing I have noticed, is when there's a sunny day, after about 30min on the outside, I can feel libido goes slightly up (it's still nowhere where it should be). I wonder if it's somehow related to SHBG. Perhaps I don't have that low SHBG, and the reason I had it was because I was taking 4000iu of D3 per day? Anyway, I think I'm going to take 2000iu per day, just to have more hormonal stability and not be so variable to the weather.
I'm going to do the bloodwork, and now my last chance is calcium d-glucamerate. If total T on the bloodwork shows too high, I will also lower my daily dose. Hopefully this will allow me to continue TRT without using AIs.
Because of all these expirements, I haven't added HCG yet. I kinda cannot add it now, as it would skew with my research. I wonder how much estradiol could HCG contribute. Besides additional T, it does also make the testes produce E2, doesn't it? Could it be significant amount?
By the way, do you think it is fine if I do the bloodwork 2 hours after the shot? Is 2 hours enough for T to hit high serum levels? Now when I think about it, when I started TRT, I felt it after a few hours.Last edited by mac34; 05-27-2019 at 11:51 PM.
-
05-29-2019, 01:28 PM #19
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I got the bloodwork results. I did it in another lab, another country, and they use different units, but after converting them I'm shocked. These are the results I would expect if I stopped my TRT.
Total T: 8.15nmol/L (6.05 - 27.80) == 2.35ng/ml
Estradiol: 95pmol/l (29-194) == 26pg/ml
What I changed is that I started injecting every day, used different needles and adjusted the dosage to what I thought was the dose I need - based on some calculations and measurements.
It is hard to believe, but for the results to be wrong they would have to make a mistake on both T and E2 readings. Though I think based on my previous experience, I could feel if my testosterone was that low. About one week ago I noticed I'm getting bulked up nice, this week I noticed I look a little worse, but I didn't go to the gym for a week. With low T, I was skinny even when I was going to the gym regularly and eating a lot. Today I was in the gym and looked pretty pumped.
I hardly even found this lab here. I'm not sure if I would be able to find another one. I think a quick test would be to take some aromasin and see how it affects my state. If I have an E2 crash and feel like crap, then the readings are correct and I have to blast. But if I will feel better, then it means I'm high on E2 and T.
Edit:
But when I think about it, these readings, if they were in g/l dimension, they would be pretty much accurate to what I would expect. High range T, above range E2. While I never had E2 this low (26pg/ml). I think they messed up the units. I will withold the AI. Wait a week, if I would be getting smaller and weaker then I know it would be a problem. Otherwise it seems impossible.Last edited by mac34; 05-29-2019 at 01:40 PM.
-
05-29-2019, 05:15 PM #20
Associate Member
- Join Date
- Jan 2018
- Posts
- 172
Cyp or ent peaks at around a day after pinning. It's pretty unlikely that they messed up the units, but I guess it's possible. When I added HCG my T increased by around 10 nmol/l (there's also a study showing the same effect), so it can make a big difference.
-
05-30-2019, 12:21 AM #21
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
That's definitely something. Do you take the usual 3 x 300iu per week or a little more? Originally Posted by Ephemeral
Yeah it's just that I saw the results first, I thought they were in the old units. 100pg/ml estro is something I could very likely have, while 100pmol/l (26pg/ml) I never had, even after withdrawing cypionate without PCT, where T was at my lowest, E2 wasn't that low. T at levels of 8mg/ml is something what I would expect. T 8nmol/ml (2.3mg/ml) seems impossible, after all, I inject the same oil every day, even if I miscalculated the dosages, some of it must be absorbed. 2.3mg/ml are worse levels than I had 1-2 months after cypionate withdrawal
The lady seemed like she was new there, or if she wasn't new, she wasn't that smooth with the whole process. I wouldn't really be surprised if the machine gave her results in these units, and then she had different units on the paper
And by the way, I did the bloodwork, 2 hours after pinning, but I pin every 24 hours, so theoretically that should be the peak.Last edited by mac34; 05-30-2019 at 12:24 AM.
-
05-30-2019, 09:07 AM #22
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
What were the lab results before you converted the units ? The conversion formulae are finicky
I no longer check my inbox. If you PM me I will not reply.
-
05-30-2019, 02:06 PM #23
Associate Member
- Join Date
- Jan 2018
- Posts
- 172
Yeah I was taking 250 IU E3D which is 875 per week. Do u get your gear from a pharmacy? Originally Posted by mac34
-
05-30-2019, 11:49 PM #24
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
No, underground, but I have been using the same vial as before.
I guess the lab could be right. Maybe it takes some time to loose the muscles. I didn't have libido, which I thought to be the issue of E2, so it's hard to tell the difference to me between a low T state, and a high T high E state. Though it's still seems unbelievable to me I would have 2.3mg/ml T, for the last month I have been very intense with various stuff and don't feel like I'm lacking energy, only sleep and it doesn't stop me.
But the reason I say the lab might be right, I did a dumb experiment last month. I took the syringe I have been using to inject 0.1ml of oil E2D, draw water and re-injected it to the new high precision syringe. I have done it numerous times and the average was that 0.1ml in the old syringe == 0.065ml in the new syringe. I also tested once with 0.5ml == 0.43ml. And I have adjusted my dose around that. So I re-tested today, and transferred water from same high precision syringe to another high precision syringe and the loss was similar.
So I have been injecting 0.03ml every day, instead of 0.05ml = 40% less gear.
Though it still doesn't makes sense for T to be below the scale. Maybe there's some critical point where there just must be a certain amount of gear to be processed by the body and just splitting the dose in half is not enough, because there's a certain offset that will cause to waste the gear. E.g. let's say I inject 0.01ml, the loss is 0.004ml . Now I split the dose in half, I inject 0.005ml, but the loss is still around 0.004ml and I inject next to nothing? What do you think guys? I guess it could make a little sense.
Seems like the only sure fire way is to never switch the gear concentration and syringes. I have a new vial of 250mg/ml so as I try to find the new optimal dose, I will start with that vial and probably stick to that concentration if I can. Though it will be tough to do it without reliable bloodwork, I will have access to in a month. I would start with 0.04ml ED of 250mg/ml (10mg) per day, but if my offset theory is correct, then I should be injecting a little more.
-
06-06-2019, 01:23 PM #25
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Yep the results were correct. Took 1/4 of aromasin pill one week ago and definitely felt it - in the bad way. Then increased the gear dose, felt it as well. Now I will need to wait another month of trying this, and see how the results come up. I have also added the calcium d-glucaminate, hope it will help keep my E2 low as well.
-
07-05-2019, 01:02 PM #26
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Is it possible that after regular taking aromasin I could have crushed my E2 and bring SHBG even lower - which resulted in crazy testosterone metabolism?
My hair falls out more than ever, yet I did a bloodwork, 48h after the shot (just after the next shot), and my T was at the low end of the scale. I was wondering why did I got so skinny in the recent 1-2 weeks. Now I looked at the T results - no wonder. I did test my SHBG too, and it was almost the same as the last reading - 14nmol/l, but it was a few days since I ate examestene chunk
Maybe it's a good time to call it quits and try chances with recovery. It seems like I'm not made for synthetic hormones. I could feel my balls wake up sometimes after taking examestene (I don't take hcg ) - so the hpta might be in good state.
-
07-05-2019, 08:43 PM #27
New Member
- Join Date
- May 2019
- Posts
- 3
Dude I'm just gonna come right out and say it the way you take you test is completely useless, you take the tiniest of amounts and expect your body to react to it, that is stupid, your body breaks shit down and will only absorb so much so the amount you are putting in is pointless. You are making it far more complicated than it ever needs to be. Originally Posted by mac34
Sent from my SM-N950F using Tapatalk
-
07-07-2019, 02:21 PM #28
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
2 days later I feel and look way better - with the same dosing. It must have been the E2 crash and low SHBG.
Given that I'm at point 0 again, I will try to run daily dosing again - this time increase it a little bit and test weekly to see if I'm on the right track. I will also finally add hcg . Let's see if I can get without an AI, but I will still use some aromasin from time to time if I notice E2 goes up too much. For now the goal would be to get the right dose to have the total T at some fixed point, consistently.
I figure Arimdex would be a better choice for E2 control on TRT, but Aromasin is the only thing I have currently.
-
07-07-2019, 04:18 PM #29
New Member
- Join Date
- May 2019
- Posts
- 3
Again you are making it far more complicated than it needs to be dude but you clearly don't want to listen to anyone so good luck Originally Posted by mac34
Sent from my SM-N950F using Tapatalk
-
07-07-2019, 05:14 PM #30
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
DIM and Masteron should be used before touching an AI. It's a very harsh drug and can cause a cascade of problems. You are making a lot of stuff over complicated.
Do the following:
30-40mg of Test E, C, or D on MWF
300-400IU HCG on MWF
400mg DIM Every day
25mg DHEA with last meal of day
Vitamin D3, dosed at 35IU per lb of body weight
500mg Magnesium
100mcg Vitamin K2
Run that, don't change the doses, don't add or remove anything.
You are not running a proper HRT program which is why you have this cockamamie idea that your body isn't meant for synthetic hormones.
You are creating more problems than you are solving with your current mindset.Last edited by Windex; 07-07-2019 at 05:27 PM.
I no longer check my inbox. If you PM me I will not reply.
-
07-07-2019, 05:30 PM #31
New Member
- Join Date
- May 2019
- Posts
- 3
Thank you, though this bloke doesn't even acknowledge what anyone says even though we're trying to help Originally Posted by Windex
Sent from my SM-N950F using Tapatalk
-
07-08-2019, 07:06 PM #32
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I appreciate the suggestions guys. I know I have screwed up with aromasin and HCG . And yes, the doses were far too low when I wrote one month ago. This time though I'm pretty sure it was aromasin that wrecked my hormones.
I'm switching back to daily injections, but this time I will monitor the levels every week and adjust the dose properly. I also did my first hcg shot today. I didn't feel anything though yet, hope it's good.
All I'm trying to do is to minimize 2 side effects. Hair loss and elevated E2. I wished I could do a standard HRT protocol and not have 2x the estradiol I should have. Running daily injections + the supplements seem to be the best shot at it. Let's see how it goes.
And going back to my first post in the thread, I ran 20mg EOD, so that was 70mg per week - which shoot my test levels slightly above the upper natural range. And 2x the E2 levels I should have. So it's just seems my response to this is a little bit different than in average person. Going with a standard hrt protocol, these issues would be even larger.
-
07-09-2019, 05:47 AM #33
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
What you fail to understand is Test + HCg is not a proper HRT program.
the sad thing is if you were capable of listening you wouldn't have any hair problems or estrogen problems.I no longer check my inbox. If you PM me I will not reply.
-
07-09-2019, 08:11 AM #34
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
I understand that DIM could help with estradiol problems, but what is the supplement of those you listed which could help me with the hair loss? I take a vitamin complex and 100mg of magnesium per day. Originally Posted by Windex
Also I didn't take D3 as I thought it would lower my low SHBG further. Isn't the point with taking D3 to lower SHBG so there's more free test?
Sorry if I sounded a bit ignorant, I'm open to learning. I will be the last to say I got it right, I just try to figure this out. Thanks.
-
07-09-2019, 06:20 PM #35
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
100mg of Magnesium is basically zero. Magnesium without Vitamin K2 is useless. Originally Posted by mac34
Vitamin D3 is the second most important hormone in your body, and DHEA is actually first.
D3 is not at all for SHBG it's responsible for hormone signalling pathways and is the single biggest deficiency in North America, more than half the popular are D3 deficient.
99.9% of Vitamin complexes are useless and given your knowledge level I doubt the one you are using is part of the 0.01%
Literally all you have to do is copy the exact program I laid out for you. Good luck ..Last edited by Windex; 07-09-2019 at 06:30 PM.
I no longer check my inbox. If you PM me I will not reply.
-
07-10-2019, 02:33 AM #36
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
Thank you. I will start taking the supplements you mentioned, including d3. I will monitor shbg levels though. Originally Posted by Windex
Can you tell me how this relates to hair loss? Like which one of these supplements would help me with it?
-
07-15-2019, 02:56 PM #37
Junior Member
- Join Date
- Jun 2018
- Posts
- 114
One week ago, I added in HCG for the first time, at 300iu MWF. I also did the daily injections at 12.5mg per day.
It felt like I finally cracked the code with TRT. Monday to Friday sex drive was very high and I got bulkier almost immediately.
But I tested T levels today and they were only at 400ng/dl (300-800) range.
I think all this has been due to HCG, the levels could be a little higher in the week (since the last shot was on Friday) and the daily T dosing didn't add much if at all. That, and that I might not need as much total T, due to my low SHBG.
I would be willing to give a go for 500iu HCG EOD without cypionate and see where it leads me, both in lab numbers, and real life results - which is the most important I think. I will still give it some time and run bloodwork day after HCG shot, to see how different are the levels, and if the sex drive sticks.
Other direction would be to find the right daily dose. 12.5mg per day doesn't do crap, but 20mg EOD gave me 700-800ng/dl. I guess the problem with the small doses is that some initial volume gets wasted or something.
I think really the best way for me would be to try a PCT. But I will run some experiments yet while I still have me hpta shutdown.

 Reply With Quote
Reply With Quote




Thread Information
Users Browsing this Thread
There are currently 1 users browsing this thread. (0 members and 1 guests)





Expired dbol (blue hearts)
01-11-2025, 04:00 PM in ANABOLIC STEROIDS - QUESTIONS & ANSWERS