


Results 1 to 40 of 49
 1Likes
1Likes LinkBack URL
LinkBack URL About LinkBacks
About LinkBacks-
08-09-2012, 11:02 AM #1
 HRT
HRT

- Join Date
- Dec 2010
- Location
- South Fla
- Posts
- 4,713
Estradiol and Therapeutic Management: What you should know.
Since this is a subject that comes up here time and time again, I decided to start this thread so we can easily refer members to this information regarding Estradiol and its therapeutic management under Testosterone Replacement Protocols.
From the beginning...
Estradiol is simply a class of Estrogen of which there are about 30 different types. Estradiol (E2 or 17β-Estradiol, or as Oestradiol) is a sex hormone. Estradiol is abbreviated as E2 as it has 2 hydroxyl groups in its molecular structure. It is known by many of us as simply E2 as its abbreviation.
Many people (even Physicians) simply call Estradiol, Estrogen.
Estradiol is the major sex hormone of interest in foundational Testosterone Replacement Therapies.
Why it Matters
There are basically two very important reasons that we need to care about Estradiol.
The first is that Estradiol is a powerful Testosterone receptor antagonist. What this means to us men is that Estradiol creates a very strong bond to the Androgen Receptors of Testosterone and renders them useless.
However, when testosterone binds to an Androgen Receptor, it activates that receptor and we get the physiological effects we're all looking for. Now, when Estradiol binds to that same receptor it blocks Testosterone from binding, yet it does not activate the receptor, so in short nothing happens.
This means that if your Estradiol serum level is high, no matter how much exogenous testosterone you take it isn't going to help you as it should because too many of your androgen receptors are now blocked by Estradiol and your Free Testosterone has nowhere to go.
Exogenous Testosterone can't do you any good if it doesn't have receptors available to activate simple enough.
Now, things can get worse believe it or not... some believe that elevated levels of Estradiol can cause the down regulation of Androgen Receptors. What this potentially means is that your body may respond to higher levels of Estradiol by creating fewer Androgen Receptors as cells are replaced in a normal regeneration cycle.
So, not only does Estradiol block the available Androgen Receptors as noted, it may cause your body to produce fewer of them in the future!
This is where many Docs get it wrong and is one primary reason why just raising Testosterone serum levels alone as a mono-therapy may not have any immediate effect on a man. It may be that the receptors have been down regulated and so there will be a need to lower Estradiol levels and increase Testosterone levels in order to get a mans body to up-regulate again and this could take some time.
The second reason we care about Estradiol in men is that we also have Estrogen Receptors and Estradiol will bind to them and cause them to activate. This is fine if you want to grow man boobs (Gynocomastia) add belly fat and get an enlarged prostate, among other things, but not so good if you want to look and feel like a healthy man.
Keep in mind, the aromatase enzyme lives in the skin and has a propensity for abdominal fat. Meaning the more belly fat you have the higher level of aromatase you will have.
Where Estrogen Comes From
Lets forget environmental estrogens here; the primary pathway for Estradiol production is via the conversion of Testosterone by the Aromatase Enzyme.
What this means is that the Aromatase Enzyme found in every mans body bonds to Testosterone Receptors and chemically synthesizes it to Estradiol (E2). Think about that all of this for a minute and realize that this conversion is a double edged sword. All in one process you're 1) losing Testosterone and 2) gaining Estradiol. Obviously this is not good healthy state to be in and one that needs to be managed correctly.
This is where drugs like an Aromatase Inhibitors (AI) like Anastrozole (brand name Arimidex - aka "adex" etc.) come into a well planned TRT protocol. An AI will bond to the Aromatase Enzyme and prevent it from converting your Testosterone to Estradiol.
Keep in mind, and many men get this wrong; but AIs do not work directly on Estradiol nor on the Estrogen receptors. It is SERM's like Clomid and Nolvadex that bond to Estrogen Receptors.
SERM's and AI's are different compounds, so don't get them confused. Nolvadex acts as an estrogen antagonist and will not stop the aromatization process. It disrupts the estrogen receptor bond formation process. So, your estrogen will rise but will be blocked from the chest receptors.
So, an AI gives us that double edged sword but now in reverse. An AI will prevent the loss of Testosterone to conversion and consequently lowers our Estradiol levels which helps keep our Androgen Receptors available for Testosterone.
Keep in mind that Anastrozole is a powerful aromatase inhibitor (antagonist) and that too much can easily cause you to push your E2 level to low. Its half life is app. 46.8 hrs so this needs to be kept in mind upon initiating a dosing schedule, especially if self-administering this product. In most all cases it is suggested to start with the lowest possible dose and titrate up based on frequent blood work, until stable levels are attained.
Less is more here! Both high and low E2 come with similar side effects such as joint pain, loss of libido, etc.
Estradiol Always Follows Testosterone
Here's where Doctors and other Medical Practitioners get it wrong; they forget that Estradiol always follows Testosterone. As your Testosterone serum levels elevate, so will your Estradiol levels.
If your Doctor is not doing something to manage your Estradiol levels (like taking an AI) then you aren't really going to get anywhere with higher Testosterone serum levels because your higher Estradiol levels are just going to cancel out any beneficial effect from the Testosterone. Like I said, your exogenous Testosterone can't do you any good if all your Androgen Receptors are all bound up with Estradiol.
For those of us with "age related" low Testosterone levels, this is a serious issue because our bodies are naturally trying to keep Testosterone levels lower and Estradiol higher by producing more of the Aromatase Enzyme.
If you're a younger man and have low Testosterone serum levels for some other reason, Aromatization may not be as much of an issue, but trust me it still matters. Keep in mind that many fifty plus year old men have higher estrogen levels than women the same age.
Fat!
Excessive body fat produces Estrogen and Aromatase Enzymes. If you're carrying extra body fat, one of the best things you can do to help your hormone balance is to lose that fat and for many other health reasons as well.
Problems Associated With Low Estradiol
What is the ideal number for you? That would be for you and your physician to decide. However, keep in mind, there can be just as many complications, if not more, by having your estradiol value too low. It is essential for men to have healthy levels of estrogen in their bodies to function properly.
Some have the mindset that lower is better, which is the wrong type of mindset. In fact, sustaining low levels of estradiol for lengthy periods of time can be downright detrimental!
Here are just some of the issues associated with having your estradiol level too low:
A feeling of being lethargic, sluggishness, and frequently fatigued.
Headaches
Depression
Dry skin and hair
Unhealthy nails
Loss of libido
Sore, achy joints
Inability to concentrate
Panic and anxiety sensations
Potential risks for osteoporosis and bone fractures
Potential cardiovascular and immune risks
In Range Does Not Mean Normal
One of the biggest and more frustrating problems you're likely to face is the problem of most Doctors believing that any blood test value that is "in range" is "normal" and therefore fine. I wish it was that simple and that goes for most if not all lab ranges.
Let's take a look at Testosterone values. The Total Testosterone reference range for Quest is 250-1100 ng/dL. But those values were formulated simply by looking at the values of everyone else who has a blood test for Testosterone let me say that again: everyone else.
What's normal for a young guy is to be in the higher end of the reference range. What's normal for an older guy is to be in the lower end of the range just normal biological processes.
So, while low Testosterone might be "normal" from a lab reference range perspective that doesn't mean it's good or healthy for that matter! I may be an older guy, but why should I be happy with lower Testosterone and elevated Estradiol levels simply because it's normal?
All men of all ages should be in the higher end of the reference range if they want to feel good, look good and perform athletically and sexually as men and grow old healthy!
The same holds true for Estradiol levels. The Access Medical Labs reference range for Estradiol Sensitive is 7.6-42.6 pg/ml but "normal" young men are at the low end of that reference range and that's where we all want to be as well.
Trust me, if your Testosterone serum levels is 250 ng/dl and your Estradiol is 42 pg/ml, you may be "in range" for both values, but you aren't going to feel good or have anywhere near the athletic and sexual performance that you would have if your Testosterone level was 800 ng/dl and your Estradiol level was 25 pg/ml.
A word about Estradiol Sensitive Testing
Unless your Doctor specifically requests a Sensitive assay the lab will default to the standard Estradiol assay designed specifically for women, which is useless for men. The reason for the difference between the two assays is the bell curve from which the test was designed sits within the normal range for women and not men.
Therefore, the hormone concentration range appropriate for adult men falls on the flat slope of that bell curve making it completely inaccurate for testing mens E2 serum levels. Always, ask for the Sensitive assay when your Doctor is conducting a blood test and testing for Estradiol.
Natural Variation in Populations
All populations exhibit some amount variation. The average height for men might be 5' 10" but we all know guys who are much taller and much shorter its just a natural part of our existence. This same variation applies to Testosterone serum levels, Estradiol serum levels, and reactions to various therapies as well were all different!
In other words, while what I've outlined holds true in general; how it specifically applys to you will vary.
Ok, that's enough rambling from me for now on this subject matter. I wrote this, with the expert help and assistance from kelkel and Vettester, as a basic primer; there's a lot more to this subject, so use this as a springboard to do more research on your own an learn.
Peace.
gd
-
08-09-2012, 11:05 AM #2
Member
- Join Date
- Jul 2011
- Posts
- 640
Great post!! Thanks!!
-
08-09-2012, 11:31 AM #3
 Anabolic Member
Anabolic Member
- Join Date
- May 2010
- Location
- Back from Afghanistan
- Posts
- 27,376
informative and well written.
so let me ask you. what do you take to control e when cruising, and what do you take to control e when blasting?
-
08-09-2012, 12:09 PM #4
Associate Member
- Join Date
- Feb 2012
- Location
- Ireland
- Posts
- 447
Nice one Gd finally have something to show my doc on low e2.
-
08-09-2012, 12:12 PM #5
 Associate Member
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Bravo Gdevine .Well done.I may just pass this along to my doc too.Stickie ?
-
08-09-2012, 02:27 PM #6
 Associate Member
Associate Member
- Join Date
- Jun 2012
- Location
- Philly, PA
- Posts
- 210
Thank you for writing this GD. Very good information.
Would it be inaccurate to say, "If you are measuring, total estrogens, or even estradiol non-sensitive, you are wasting your money and time"? Or is that too strong a statement. My doctor, for instance, measures total estrogens, should I tell him to stop because I don't want it?
-
08-09-2012, 04:33 PM #7
HRT
- Join Date
- Dec 2010
- Location
- South Fla
- Posts
- 4,713
Not inaccurate at all. Originally Posted by xtitan1
Originally Posted by xtitan1

Read the description as to why the standard E2 assay compared to the sensitive are different.
Yes, it would be a waste of money and you won't get an accurate assessment of your E2 serum levels which could mean a wrong protocol.
-
08-09-2012, 04:37 PM #8
 Associate Member
Associate Member
- Join Date
- Oct 2011
- Posts
- 210
Do you think there's an ideal range for E2?
-
08-09-2012, 04:59 PM #9
HRT
- Join Date
- Dec 2010
- Location
- South Fla
- Posts
- 4,713
It depends upon each male as everyone is different; but I think if you read most of the top TRT Physicians and the studies offered by LEF seems the mid to upper 20's pg/ml is the targeted sweet spot...then adjust from there.
-
08-09-2012, 05:56 PM #10
 Knowledgeable Member
Knowledgeable Member
- Join Date
- Apr 2012
- Location
- Montreal Canada
- Posts
- 1,357
- Blog Entries
- 3
vote for sticky
-
08-09-2012, 06:16 PM #11
Junior Member
- Join Date
- Jun 2011
- Posts
- 125
and thats why we need good people like the the late Chip (rip brother), cause the doc's around here will only give ya T. ( if your LUCkY), they could care less about E2, 99% of endo's are f***king clueless a**holes
-
08-09-2012, 06:47 PM #12
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
TR, hope you don't mind me chiming in on this ... Originally Posted by Times Roman
Obviously everyone is different, but in my case, when things are dialed in, I will use .25mg x 2x per week of Arimidex (Or AR's Liquidex as well) as a maintenance dose to sustain my E2 level in the range I'm at while on my protocol dose . My protocol is 120mg/wk of cyp and 250iu x 3/wk of HCG .
For blasting, again this is just me, but I have found that increasing the AI by .25mg for every 100mg of cypionate added is sufficient for sustaining my levels at/around the same range. So, for me ....
120mg of cyp = .50mg of Adex
200mg of cyp = .75mg of Adex
300mg of cyp = 1.0mg of Adex
Some might need more or less, but that rule of thumb works for me. I normally don't go over 300mg/wk when I do a blast, and I usually add around the same amount of Deca to compliment it. And to note, I'm currently on my normal protocol dosage, but not taking any AI at the moment with hopes to get my E2 in the low 30's. That's always the best range for me libido wise. I'll rerun labs again in September and see where it sits. If achieved, I'll run with my .25mg x2/wk program again.
-
08-09-2012, 07:00 PM #13
Anabolic Member
- Join Date
- May 2010
- Location
- Back from Afghanistan
- Posts
- 27,376
I'm sitting on several hundred tabs of 10mg nolva. i was thinking of taking maybe 5mg/day while cruising and continue with my exemestane while blasting. (I blast maybe twice a year). Any advice for the nolva, or do you think it would be better to stick with the exemestane while cruising? Originally Posted by Vettester
I haven't thought this all the way through yet, since just recently with the ai, so open for suggestions?
-
08-09-2012, 08:53 PM #14
 HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
If you can avoid the AI completely you're always better off. Unfortunately the majority cannot do that. Curious, what does your E2 level run at while cruising normally TR? I don't think I'd go below 10mg of Nolva if I was going to try that, in conjunction with frequent BW to monitor E2 levels and see how it works for you. Nolvadex , and you need no explanation, is a tremendous asset to have around.
My protocol is pretty much the same as Vettes. Only difference I do not need an AI as my E2 runs low at 15 - 16. This was determined by 3 or 4 monthly E2 tests in a row. If I go above that dosage I need an AI. Very sensitive nips here and I will always have Nolva on hand. My doc even says there are people that run low but can still have sensitive issues.
-
08-09-2012, 09:28 PM #15
Associate Member
- Join Date
- Jun 2012
- Posts
- 415
Excellent post, best info on e2 I have seen. Need to sticky. I still do not trust lab corp sensitive essay. I lean toward the reg. E2 test when I test through privatelabs.
-
08-09-2012, 10:30 PM #16
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
TR, unfortunately Nolva won't inhibit the aromatase enzyme to reduce & control your E2. Being a SERM, it will block estrogen from attaching to breast tissue receptors, thus making it a great compound to help mitigate gyno, and even the receptor sensitivity sides of estrogen rebound. However, to control the actual E2 serum levels, you will need to stick with an AI like the Exemestane, or an Arimidex type compound. Originally Posted by Times Roman
For me, I only needed Nolva one time (less than 2 weeks), which was when I went through a bout of estrogen rebound after my E2 had crashed. Personally, I don't think Nolva is needed in a HRT regiment unless you're having some sensitivity issues with the nipples (as noted by Kelkel) and/or seeing some possible gyno, or if for some reason your E2 ends up in the tank and you might be dealing with some upcoming E-Rebound. As Kelk mentioned, start with your labs first. You might have to run a few back-to-back consecutive labs (while on cruise and blast) to get the dosages dialed in, but IMO it's well worth it in the long run as Kelkel will attest.
It's always good to have some Nolva on hand though ... So don't get rid of it by any means.
-
08-10-2012, 04:37 AM #17
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Gdevine you mentioned liquidex.Is it a liquid?How do you take it if it is?And how much how often?I am on test cyp 50mg every 3.5 days so when would I take liquidex and how much to start on?I still haven't convinced my doc to prescribe an AI so am thinking about taking matters into my own hands.Also will it show up in a negative way on a drug screen at work?I am in a safety sensative job and get tested constantly.By the way my E2 is 67.
-
08-10-2012, 08:06 AM #18
 Associate Member
Associate Member
- Join Date
- Aug 2010
- Location
- NORTH NJ
- Posts
- 288
Thanks for taking the time and write this up for us gf !
-
08-10-2012, 08:07 AM #19
Associate Member
- Join Date
- Aug 2010
- Location
- NORTH NJ
- Posts
- 288
Ummmm ... That's " gd" my phone love auto correcting me
-
08-10-2012, 05:19 PM #20
 HRT Specialist ~ Knowledgeable Member
HRT Specialist ~ Knowledgeable Member
- Join Date
- Oct 2011
- Posts
- 1,985
- Blog Entries
- 27
Good post, it is important for men new here to know that e2 is not the enemy!
Also, I would like to point out that the sensitive test for Quest Diagnostics is called ultrasensitive.
For most docs, you will need to hammer it into them that the standard estradiol (e2) test is a waste of your time and money.
-
08-11-2012, 09:30 AM #21
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Gdevine comments on my post above?Anyone else have experience with liquidex ?
-
08-11-2012, 10:51 AM #22
Junior Member
- Join Date
- Jul 2011
- Posts
- 98
Are there risks associated with Arimidex other than driving your E2 too low? I understand less is more. Are there specific reasons Drs are reluctant to prescribe other than not an approved use for men. Thanks.
-
08-11-2012, 07:19 PM #23
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
Originally Posted by Oldhighlander
I don't think GD made any comments on Liquidex (maybe it's somewhere and I didn't see it), but I made mention of it in post #12. Originally Posted by Oldhighlander
Yes, I have experiences with several forms of the AI's, including Liquidex, which is just Anastrozole / Arimidex in liquid form. The dosages with Liquidex can be administered exactly the same as you would with the pill or capsule form of this medication. AR-R 's Liquidex comes in a 30ml bottle, and its dosage strength is 1mg/ml. Its taste is pleasant and can be administered with an oral syringe, which AR-R always includes in the package with your order.
As mentioned to TR, my normal maintenance dose is .25mg x 2/wk. You can read the details of my protocol in post #12. Dosage amounts will vary in each individual, so it's essential that you keep a close eye on it with maybe running some labs for a few months til you get it all dialed in.
This compound has risks, just like anything would, and there's always a chance that you could have some sort of reaction (usually minor if any) when taking it. For me personally, I've never had any problems what so ever. There's some that have complained about it negatively effecting the lipid panels, and even some that state that it diminishes their libido. IMO, I think most people will see a drop with libido only if you skew your E2 level too low, or maybe drop it too fast in a short period of time. If it takes 3 months to get it dialed in, GREAT!! That's better than crashing it in 2 weeks and going through all the garbage that comes with that.
Your E2 score is at 67. I'm curious what reference range was used in your lab assay? Regardless, we know it's a bit high and will need to come down. If it were me, and it again this is based just on my own personal experiences, I would first try .25mg of the Liquidex. If you don't develop a fever, rash, vomiting, diarrhea, yellow skin & eyes, dizziness, vaginal discharge, or any other weird symptom, I would then take another .25mg in 3 to 4 days. If all continues well, I might look at trying just a little more; possibly .30mg or .35mg x 2/wk for 1 month, then run your E2 lab.
If your E2 has slightly dropped after running labs, you might need to slightly increase your AI dosage, or if it has dropped to <45 in 1 month or less, you might need to taper back a bit to avoid the risk of dropping too fast, or worse yet, crashing! I think it was Bass that crashed pretty quick with a dose that wasn't all that high, so it does happen. Again, it takes a little bit to get it dialed in, and best to go a little slow and let it gradually get you in the zone you need to be in. Whether that zone is in the low or mid 20's, or somewhre in the 30's, that will be dependent on how you feel and respond.
As far as your job goes, unless they're specifically testing for estrogen inhibitors, you shouldn't have any problems. Liquidex doesn't have any anabolic characteristics, and I've never heard of anyone ever getting screened with it, unless possibly in certain sports where it might be considered as a catalyst to increase free testosterone .
To answer you on the best time to medicate with Liquidex ... I personally find it best to administer it one (1) day after my cypionate injections, which I do SubQ BTW. The half life of Liquidex is/at around 48 hours, depending on how well your body metabolizes the compound. Testosterone cypionate has a half life of 7 to 8 days, but usually peaks closer to three (3) days. Not that you have to get this down to the exact minute, but usually running your AI at some point the day after your cypionate shot will help ensure that it reaches its best efficiency level at/around the same time that your testosterone serum levels are also peaking; all maximizing the efforts of your E2 control.
-
08-11-2012, 08:32 PM #24
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Vettester you are correct,it was you.My bad.The range is 7.63-42.60 pg/ml.I am currently injecting 50mgs of test cyp every 3.5 days so my protocol with liquidex would look like this.Test cyp 50mgs sunday evening,liquidex .25mgs monday evening,test cyp thursday morning,liquidex .25mgs friday morning.Does that look right?Then blood work in a month and adjust accordingly.Thank you so much for responding.It is a big help.I have been trying to get my doc to prescribe an AI but she said she wasn't comfortable doing it because she has never used it for this purpose.I gave her print outs from Dr. Crisler and a few others that were suggested and have been waiting for an answer.I called the office friday and left a message.So when she calls back I will know what I have to do if she doesn't prescribe.I have been trying to be patient and I think I have but enough is enough.
-
08-11-2012, 09:06 PM #25
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
^^ Yes, I concur with your suggested protocol. Thanks for confirming your assay is indeed the Access Medical Lab standard with the reference ranges you provided. It may take a little more compound to bring your score down to an acceptable level, but as stated, start slow and get familiarized with the compound, then the adjustments can be made to your protocol.
If anything, this might be a good opportunity to get a new thread going for yourself, where you can post all of your current labs, including lipids, hormonal, etc., then we can dial-in with you as you progress. I know many members, including myself, that will want to subscribe and help you see this through.
Dealing with a female doctor on some of this can sometimes be difficult. There are some decent A4M certified female doctors, so it's not as if they don't exist, but I personally know what you're up against with the family medicine practitioner when talking about things like "Arimidex for men". Keep in mind, your doctor has probably been schooled on the concept that an AI, like Arimidex, is a medicine that would be only prescribed for treatment for women with breast cancer. They get this data fixated in their heads, then some blokes like us come walking in the door and say we want an AI to support our HRT programs. Hopefully, some will keep an open mind with reading the reports from Dr. Crisler and others that know the benefits.
-
08-11-2012, 11:48 PM #26
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Very well said Vette....
-
08-12-2012, 08:42 AM #27
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Vettester I am a little hesitant to use the liquidex because of my job.I really don't think it is the kind of thing they are looking for but I really don't know.When the doc calls I might try a little threat so to speak.If she doesn't prescribe I am going to tell her that I am going to try a black market product (not sure if it's black market or not but it will sound more dramatic to the doc) because I think it is that important to get my E2 in a good range for my health.Then see what she has to say.I really feel that if she doesn't prescribe then taking test could do more harm then good for my long term health.Not to mention all of her other patients that she is treating with test.And I am pretty sure there are alot.When I went in to learn how to inject myself I was the fourth one that day.I am not really showing any bad symptoms other then holding water.I am on a diruretic for blood pressure now and still holding water.I was border line high and she gave me a very low dose as a precautionary measure.Would getting my E in line help me to not hold water and possibly dump my BP med?I have really got serious about my overall health when I started TRT.I always trained and competed in the Highland games and some strongman stuff but wasn't real good about my diet.Now that I am on TRT I have cleaned up my diet(lost 65lbs so far)and am training harder then ever.My weight has gone down and my training weights have gone up.All of my numbers have gotten better (triglycerides,BP)I am at the point to where I think I can start dumping meds I hope.One more thing to talk to the doc about.
I also wanted to ask about your experience with blast and cruise.Can you explain the difference between the two and what is the end goal with them?Once I get dialed in I think I would like to give it a try.I have made some real good gains so far on just TRT dosing.Is it physcological or is that small of a dose of test that powerful?I have really changed my body comp and am not sure if it is because of hard training,good diet or how big a factor the test is.The changes have motivated me to train even harder.I am hitting life time personel bests in the gym and in competitions.That in turn makes my outlook even better.
I will start a thread on my journey at some point soon.Should I post everything from my baseline to present?It is interesting to look at my numbers and see how they have changed over time.Where would I post something like that?Here or is there a special place forthat kind of thing?
Thnaks again everyone!It is great that a bunch of guys I have never met will go out of there way to help a perfect stranger.Hell there might be hope for this planet yet!
-
08-12-2012, 11:45 AM #28
Associate Member
- Join Date
- Jun 2012
- Location
- Philly, PA
- Posts
- 210
One thing I noticed reading Shippen's book was his discussion of non pharmaceutical means of lowering testosterone , such as 50 to 100 mg of zinc daily or eating a lot of soy. His book is outdated, though, so maybe opinions on that have changed. Nonetheless, wouldn't those methods be preferable for minor estradiol elevations or in situations like the above poster's where getting an AI prescribed is proving difficult?
-
08-12-2012, 12:37 PM #29
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
Oldhigh- Yeah, it would be best at this point to start you're own thread. We're starting to divert off course when talking cruise and blast, and other things attributed to your program. If you get a new thread going, put all your details in it, I'll chime in ...
xtittan - The zinc regiment could be tried, but I would still stress for labs to be taken to see just how effective it is. IMO, there's going to be no better route to go than using an AI when a person's E2 is in the 60's, and they're currently on a TRT protocol.
-
08-12-2012, 01:07 PM #30
Associate Member
- Join Date
- Jun 2012
- Location
- Philly, PA
- Posts
- 210
Roger that!
-
08-12-2012, 04:06 PM #31
Associate Member
- Join Date
- Feb 2012
- Posts
- 173
Xtitan 1 I tried zinc,L-carnitine and whatever else has been suggested and it didn't work for me so I see no other alternative but an AI.
Vette I will start another thread with all my particulars in it from day one baseline readings and up to the present.I guess it will almost be a blog.It has been an interesting journey so far.I hope people will read it and chime in with suggestions.Knowledge is power!
-
10-25-2012, 03:40 PM #32
New Member
- Join Date
- Mar 2012
- Posts
- 4
xcraider37,Why dont you trust lab Corp "senitive essay test"?Is there another test from them thats better?Its the only lab my doctor uses:not that I've got him to give me one yet.Been over a year.Thanks in advance.
-
10-25-2012, 03:48 PM #33
Associate Member
- Join Date
- Jun 2012
- Posts
- 415
Ive decided not to fight this battle on this forum, my suggestion is to do your own research. Originally Posted by ronbowe63
-
12-09-2012, 08:41 PM #34
 Associate Member
Associate Member
- Join Date
- Sep 2012
- Location
- Canada
- Posts
- 314
Could someone expand on this? Originally Posted by gdevine
Specifically "the hormone concentration range appropriate for adult men falls on the flat slope of that bell curve"? What does that mean exactly?
Is using the normal "female" test really "useless" as stated, or just less useful? I ask because in Canada I have never heard of the "sensitive assay" here. Although there are different methods used. Perhaps "sensitive assay" has a different name here?
-
12-09-2012, 08:56 PM #35
HRT
- Join Date
- Dec 2010
- Location
- South Fla
- Posts
- 4,713
"...eating a lot of soy"
Soy, like Flax, is an estrogen mimic and men should stay clear of both.Last edited by steroid.com 1; 12-09-2012 at 09:00 PM.
-
12-09-2012, 09:04 PM #36
HRT
- Join Date
- Dec 2010
- Location
- South Fla
- Posts
- 4,713
Women's serum levels of estrogen if in a man would kill them. Originally Posted by junk2222yard
Now think of a bell curve where most most estrogen assays, by default, are designed for women.
How accurate than do you'd think it would be for a man who has a tiny fraction of the amount of estrogen serum levels of women?
Help?
-
12-09-2012, 09:15 PM #37
Associate Member
- Join Date
- Jun 2012
- Location
- Philly, PA
- Posts
- 210
Originally Posted by junk2222yard
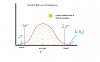
The part you are quoting is referring to a concept that is at the core of statistics. Wikipedia link if you are REALLY interested: http://en.wikipedia.org/wiki/Normal_distribution . If you don't feel like reading that (and it's not really worded well for someone who isn't familiar with the subject), I will try to explain. If LabCorp takes a bunch of women's E2 numbers (because women usually are the ones who get this test done for breast cancer screenings, menopause, and a whole plethora of reasons), they can take that data and put it on a graph called a probability density function. That allows LabCorp to see probabilities that a given woman will fall in a given range of E2 numbers.
Now it turns out that in general, one of the most common things you see in these graphs is that the data forms a bell shaped curve, where it extends out barely above the x-axis in either direction, and at some point around the mean, or average of all the numbers, it forms a raised portion. That gives it a bell-looking shape. LabCorp then picks two equally distant E2 numbers out from the center of that bell so that they get a 95% probability, and that's where the E2 reference range comes from. Yes that 95% number is totally arbitrary and is why reference ranges can sometimes be totally useless, but they at least give you an idea of where normal people are at.
If you instead were to go through the same process for E2 numbers drawn from men, the bell curve would be WAYYY smaller and way to the left of the women's bell curve (out where the bell curve has gone flat). In other words, the majority of men get E2 results that are in much smaller quantities and are over a much smaller range than women's . The normal E2 test's accuracy is designed for women. LabCorp doesn't have to spend extra money being super super accurate because 10 or so units one way or the other for a woman doesn't really make a practical difference when trying to diagnose her with a medical problem. That inaccuracy really actually doesn't seem very significant on the large bell curve that E2 has for women.
For a man, however, that could be very significant.
The solution? Get the "ultrasensitive assay" which is a more expensive test where LabCorp makes sure it is more accurate in getting your E2 number. You wouldn't want to get the normal E2 test because it's based on statistics from women who have larger ranges of E2. You might change, or fail to change, your AI dose because you were given bad information.
As far as Canada is concerned, I don't live there so I don't know what labs you have there. The "ultrasensitive assay" is just LabCorp's marketing term for that specific test. Each lab will call it a different thing. Which one it is, or if the lab even offers it, depends on the lab company. Basically you are just looking for a more accurate E2 test than what they normally prescribe, because it really usually only gets prescribed for women because most doctors are idiots when it comes to E2 management in TRT.
Hope that helps. By the way, I have found that my E2 (regular test) has been very accurate and Shippen does not bother with the ultrasensitive assay, but that's just anecdotal.
-
12-09-2012, 09:46 PM #38
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
XT that is extremely well written! Knowing you I bet you have a chart somewhere as well!
kel
-
12-09-2012, 10:19 PM #39
Associate Member
- Join Date
- Jun 2012
- Location
- Philly, PA
- Posts
- 210
Originally Posted by kelkel
I knew I was forgetting something...
-
12-10-2012, 02:06 AM #40
Banned
- Join Date
- Aug 2009
- Location
- Californication
- Posts
- 5,656
LMAO!! That chart is excellent! Originally Posted by xtitan1

 Reply With Quote
Reply With Quote
Thread Information
Users Browsing this Thread
There are currently 1 users browsing this thread. (0 members and 1 guests)






First Tren Cycle (blast)
Today, 11:29 AM in ANABOLIC STEROIDS - QUESTIONS & ANSWERS