


Results 1 to 40 of 44
 27Likes
27Likes LinkBack URL
LinkBack URL About LinkBacks
About LinkBacks-
04-30-2020, 09:25 AM #1

 New Member
New Member

- Join Date
- Oct 2017
- Posts
- 38
Adding nandrolone to TRT
My TRT doc just recommended adding 90 mg/week Nandrolone to my TRT protocol of 120/mg Test-C. Initially asked about using a blend of Test E, C and nandrolone, instead of just Test-C to see if it will help my knee pain. Rather than switching to a blend, she wanted me to keep my current protocol dosage and add in the nandrolone.
My labs from Feb showed:
Total Test: 978 (normal range: 264 - 916 bf/dL)
Free Test: 26.3 (normal range: 8.7 - 25.1 pg/mL)
Estradiol: 34.9 (normal range: 8 - 35 pg/mL)
Should I be concerned with the addition of nandrolone as I am already above normal range for testosterone and right at the top of the range for estrogen? I take 0.125 mg anastrozole twice a week and DIM 200 mg daily - like for my estradiol to stay at its current level.
I havent dabbled with cycles - just my TRT protocol to date. Mainly hoping for joint relief but wont be disappointed if it helps put on more muscle.
Be interested to hear experiences from those with nandrolone as part of their TRT.
-
04-30-2020, 09:40 AM #2
 HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Your numbers look great currently! I assume when you do your blood work you do so at trough level. So know that your levels would be much higher earlier in the week assuming you are on a weekly protocol. If you are on a split protocol of twice weekly shots then there's obviously less of a trough.
Adding deca will not raise your T levels. Basically because deca is not T and vice versa. What you will have to do moving forward though is to make sure your doctor uses the LC/MS-MS testosterone testing methodology for accurate results. Otherwise using the default ECLIA method will give skewed (higher) results as deca is listed as an interference substance with the ECLIA methodology. Make sure your doc knows this as most do not. it has to be written on your blood work script otherwise they default to the ECLIA.
I'd also consider dumping the adex if possible. It's just not a healthy item long term. Estrogen does not have to be "in range." Most men will have a better libido with estrogen being higher rather than lower. Estrogen is also quite anabolic . You'd be better off dropping your test dose slightly to compensate if you feel the need. Knock off 20 mgs as you won't notice it anyway.
Deca will definitly help with joint relief although it will take some time. I've been on it for years now and would not ever consider coming off of it. Plenty of guys here are. It's also quite refreshing to see that you have a forward thinking doctor as well. Deca really doesn't aromatize to any extent (if at all) worth worrying about.
Let us know how you make out please!-*- NO SOURCE CHECKS -*-
-
04-30-2020, 10:12 AM #3
New Member
- Join Date
- Oct 2017
- Posts
- 38
Thanks Kelkel, I was hoping you’d be one to respond.
Those levels are as much of a trough as I can get - I swapped to sub-q shots and inject my test three times per week and hcg three times per week but on alternate days.
Slowly been walking the AI down and still hope to get rid of it. I dropped it from 0.25 mg to 0.125 mg after my blood work last fall, in addition to going to more frequent smaller sub-q injects, so I wanted to wait to see my BW from Feb before making further tweaks.
I will be sure to mark a reminder on the LC/MS-MS method although I bet she is aware.
How long should I expect before I notice it in my joints? Doc is running a 3 month trial and we will talk to see if it’s something we want to continue with.
We also threw around running some BPC-157 but my budget only allowed for me to pick one or the other.
Thanks again
-
04-30-2020, 10:30 AM #4
BANNED
- Join Date
- Nov 2017
- Location
- Bragging to someone
- Posts
- 8,550
adding therapeutic dosage of nandrolone is going to give you anti inflammatory benefits ,, prevent disease, help arthritis pains, and enhance your recovery .
your doctor is right on point , imo
-
04-30-2020, 10:31 AM #5
Banned- for my own actions
- Join Date
- Feb 2014
- Posts
- 1,957
I keep 100mg of deca in all the time (usually about 3 weeks after I take it out I regret my decision). I would say within 3 weeks to a month youll start to notice the anti inflammatory effects on your joints at that dose (it occurs faster if I frontload a bunch, but thats not necessary if youre not having issues) Originally Posted by Tim1985
Originally Posted by Tim1985

-
04-30-2020, 11:28 AM #6
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by i_SLAM_cougars
Yep. Been there, done that. Never again.-*- NO SOURCE CHECKS -*-
-
04-30-2020, 11:56 AM #7
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Tim1985
Oh let me know if she's aware of the correct methodology. I still bet she isn't aware even though she seems very on point with things! I would think you'd feel it in a month or so. Much better option that BPC which in my opinion is more for tendons/ligaments than joints. BPC is cheap though on peptide sites.-*- NO SOURCE CHECKS -*-
-
05-01-2020, 09:20 AM #8
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
Do you know if it's Bayer amps? And is it covered by your insurance ? Only downside to scripted deca is price if you are going to be paying out of pocket
I no longer check my inbox. If you PM me I will not reply.
-
05-01-2020, 10:54 AM #9
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
I've had it scripted in the past and had to get it from a compounding pharmacy. Horribly expensive, like 300 per 10 ml vial. I was able to submit it to insurance for a while but eventually they wouldn't reimburse me. Originally Posted by Windex
-*- NO SOURCE CHECKS -*-
-
05-01-2020, 05:31 PM #10
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
Kel hit all the points I was going to make!
1) Drop the AI. Most guys don't need it and it can screw with you libido, erections, and GH secretion. Guys need E2 too and it you keep T in range at both the peak and nadir (trough), E should also remain in range.
2) Use the LC/MS test method for T while on Nandrolone because the direct method uses an antibody that has cross-reactivity with other anabolics like nandrolone and will read a false high number.
3) It will probably help with the joint pain and give you a nice anabolic boost for building muscle. Nothing crazy at that dose, but noticeable. Ver recently, I started blending in nandrolone ( faster acting NPP rather than DECA ) into my T. I use a slightly higher does of both T and nandrolone than you do, which amounts to 130mg T-cyp/week and 117mg NPP per week. During this experiment, I switched to a daily dosing schedule. I noticed an almost immediate boost in the weights that I was able to use (NPP is very fast acting). I'm in my 3rd week now and I'm also noticing an improvement in elbow pain from a surgery I had a couple years ago. This, despite the heavier weights. Usually increased exercise volume aggravates the elbow. I'm becoming a believer in the regular use of moderate levels of nandrolone in a TRT protocol!
4) The one thing I'd add is that you don't want to go too high on the nandolone dose without carefully watching and controlling E2. At this dose, you need not fear, but nandrolone has some progesterone-like activity. Progesterone + High E2 is a recipe for gynecomastia . So, keep T in range with moderate frequent dosing (like you are doing) and also use nandrolone in moderatation (like you are doing) and you should be fine.
-
05-03-2020, 11:31 AM #11
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Good to see you YG%%!
Let me know your thoughts on nandrolone after some time please!
Saw this on estrogen the other day. You'll find it interesting:
https://jayccampbell.com/blog/estrog...ers-are-dying/-*- NO SOURCE CHECKS -*-
-
05-05-2020, 09:03 AM #12
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
Hi Kel, Originally Posted by kelkel
Been busy at work, so not a lot of time to post.
Regarding E2, the normal guy on TRT should not fear E2, even if it becomes slightly out of range. E2 is made from T, so when T goes up so will the rate of conversion to E2. It's a simple mass-action enzymatic conversion. The more T you feed the aromatase enzyme, the more E2 you will get. The simple solution for guys on TRT is to move to lower and more frequent dosing of T so that your peak and nadir levels of T always stay within or close to the "normal" range. E2 will follow.
The problem is when guys just don't get this and approach TRT with a 'more is better' approach, or use old school protocols of once weekly or (God forbid) once ever 2 week protocols. With these old school protocols still prescribed and promoted by dinosaur doc, comes huge spikes in T at the beginning of the injection cycle in order to keep nadir levels within range at the end of the injection cycle. Therein comes the huge spike in E2 at the beginning of the cycle which takes some time for the body to clear, and then you do it all over again but this time building on the uncleared levels of E2 from the prior injection cycles. It's a hormonal roller coaster ride to hell!
Guys are paranoid of E2 because of bro talk in the locker room. Bodybuilders sometimes have problems with gynecomastia and they blame it on E2. Which has some basis in reality, but the real truth is that they are often stacking many anabolic hormones on top of each other and at the base of these stacks are way higher doses of T than we use in TRT. The huge doses in T (e.g., 300-500 mg/week), cause spikes in E2, which of and by itself is not horribly bad, but many of the other synthetic anabolic agents they stack with the T (e.g., nandrolone) also have affinity to the progesterone (P4) receptors in the body. High E2 + P4 is a recipe for gynecomastia. This is what happens in the 3rd trimester of pregnancy when the placenta takes over hormone production in women. It pumps out huge amounts of both of these hormones in order to prepare the breast tissue for lactation, so there is rapid development of the mammary glands. Throw in high levels of prolactin (or in the case of pregnancy placental lactogen which has prolactin-like activity) and you begin to lactate. Many of the synthetic anabolics also have a propensity to bump up prolactin levels. I've seen videos on the internet of bodybuilders lactating. It's not pretty!
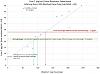
Coming back to nandrolone, it's new to me Kel. I've only been experimenting with it for about 2+ weeks to see if I can get some relief from my elbow injury from 2 years ago. It seems to be working well. The moderate anabolic boost is an added perk too, but not my primary motivation (I've got more than enough muscle mass from 20+ years of weight lifting). I've been experimenting with various doses of T over the past year too in order to optimize my Free T without having to use synthetic anabolics (e.g., stanozolole or Oxandrolone (Anavar )) to suppress my high SHBG. I've selltled on 125 to 140 mg/week E3D protocol as my optimal protocol. This keeps my E2 from going way out of range and bring my Free T within the Target range.
Can't remember if I've posted the graph of my T range-finding experiment in this forum. Here is is:
-
05-05-2020, 10:33 AM #13
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Youthful55guy
above...and as always, great to see you here.-*- NO SOURCE CHECKS -*-
-
05-08-2020, 10:52 PM #14
New Member
- Join Date
- Oct 2017
- Posts
- 38
I am going through a compounding pharmacy and paying out of pocket. They charge $150 for a 10 mL vial or $80 for a 5 mL would based on Kelkel’s pricing, sounds like I’m getting a fair price.
-
05-09-2020, 09:41 AM #15
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Tim1985
Cheap compared to what i was paying. Even though I was initially getting reimbursed it irked me. Just get my own now. Much easier and cheaper. Eventually you'll be doing the same!-*- NO SOURCE CHECKS -*-
-
05-09-2020, 12:40 PM #16
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
Same here. TRT hormones and supplies are dirt cheap compared to most other drugs and even supplements. I don't even bother to submit for insurance coverage and deal with their silly rules. I get most of my stuff by script and fill it at a local compound pharmacy. Since I use slightly higher levels of T than are prescribed, I do bolster my supplies through overseas purchases but I only purchase branded hormones. Usually, I stick with Alpha Pharma. I get a little extra T-cyp and my nandrolone from them (don't have a script for nandrolone).
Here's my annual supply cost excluding the overseas purchased stuff:
PRIMARY HORMONES (all prescribed) = ~$907/year = $2.48/day
Testosterone Cypionate -Pizer branded Depo-Testosterone 200mg/mL - Local Pharmacy $63.36/10 mL. At prescribed dose of 0.2 mL E3D = 50 doses/vial = 150 days of treatment = $0.4224/day = $154.18/year
HCG - Merck branded PREGNYL - Local Pharmacy $127.01/10,000 IU = $0.012514/IU. At 1050 IU/week (current dose 2X more than prescribed) = $13.34/week = $693.47/year
Syringes (for testosterone) - 122 (28G 1/2 inch) 1 cc insulin syringes/year. Currently use Easy Touch brand from https://www.totaldiabetessupply.com/...g-1cc-1-2-inch. $14.45/100 = $0.14 each = 122 X $0.14 = $17.08 /year
Syringes (for HCG) - 156 (31G 5/16 inch) 0.5 cc insulin syringes/year. Currently use Easy Touch brand from https://www.totaldiabetessupply.com/...-5cc-5-16-inch. $13.99/100 = $0.14 each 156 X $0.14 = $21.84 /year
Doctor Visit (copay) = 1/year at $20 = $20.00 /year
Labs = $0 (no copy)
-
05-10-2020, 03:36 PM #17
 Senior Member
Senior Member
- Join Date
- Jul 2004
- Location
- CT
- Posts
- 1,222
My Dr. said he has to write the RX as one inject every 2 weeks as that is the current standard medical industry protocol. But he tells me to take 1/2 dose every week. Originally Posted by kelkel
-
05-10-2020, 05:41 PM #18
 Castle Power
Castle Power
- Join Date
- May 2015
- Location
- Norway
- Posts
- 7,496
Just take one tbl DIM morning AND evening. 400 mg total. I notice a big difference from running 200 and 400.
Deca at that dose will not do anything to your hormones but could very well be good for joints.
You are lucky to have a trtdoc that gives u deca!
Sent fra min BLA-L29 via Tapatalk
-
05-11-2020, 04:25 AM #19
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
Are you injecting NPP subQ or IM out of curiosity ? Originally Posted by Youthful55guy
I no longer check my inbox. If you PM me I will not reply.
-
05-12-2020, 08:27 AM #20
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
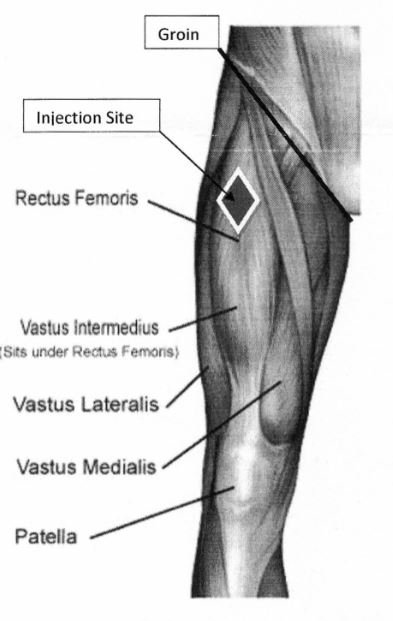
I mix it with my T so that there's just one injection per day. Difficult to answer whether it's subcutaneous or shallow muscle. I use a 28G 1/2 inch (needle) one piece insulin syringe. Inject into my upper outer quadriceps muscle. I'm about 20% BF and have some fat on my legs but not a huge amount. I can see the muscle outline even without flexing. I'm pretty sure it's shallow muscle. Here's a diagram of the injection site. Originally Posted by Windex

-
05-12-2020, 09:21 AM #21
Staff ~ HRT Optimization Specialist
- Join Date
- Mar 2011
- Location
- Arctic Circle
- Posts
- 4,286
Thanks !
A year supply of NPP is cheaper than a single Month of Deca from the pharmacy.I no longer check my inbox. If you PM me I will not reply.
-
05-12-2020, 01:50 PM #22
 Knowledge Member on Prostate Cancer
Knowledge Member on Prostate Cancer
- Join Date
- Oct 2012
- Location
- N. GA. Jaw Ja N A Cave
- Posts
- 1,946
- Blog Entries
- 1
After reading all this enlightening info , I have a question . I have LOW SHBG and from what I have read lower SHGB makes the receptors more willing to receive hormones ........ Mine is low and out of range big time ........ Is there a common reason for this ? Originally Posted by Youthful55guy
I can post BW from Late Jan is it will help but I will not be able to get more BW until the end of July ...... So that is the most recent I have and that was right before my left knee replacement . That by the way still hurts like a MF'er 3 moths post op .......
-
05-12-2020, 02:02 PM #23
Knowledge Member on Prostate Cancer
- Join Date
- Oct 2012
- Location
- N. GA. Jaw Ja N A Cave
- Posts
- 1,946
- Blog Entries
- 1
Another question please . Deca and NPP cost me the same . If I am not mistaken NPP is EOD dose . Is Deca better at 100mg a week or NPP at EOD 40mg
Test @ 40mg EOD
Tren @ 40mg EOD
Deca @ 40mg EOD
Primobolin @ 40mg EOD
NPP @ EOD 40mg
Got 2 bottles of Primo
Shit ton or Cyp
6 bottles of NPP
2 bottles of Deca
4 bottles of Tren ( love this stuff )
200 Halo Caps
So any thoughts
Have not started all of this but at peak this is the plan . Is the NPP overlapping the Deca ? are these doses small enough or large enough ?
-
05-12-2020, 05:25 PM #24
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Remember Buzz testosterone and most other anabolics will suppress shbg. Yes, some people can be naturally low as well. Only real issue with low shbg is if you have other comorbidities. Google Metabolic syndrome and that basically sums it up. And yes, low shbg means more available free testosterone as it's not bound.
-*- NO SOURCE CHECKS -*-
-
05-12-2020, 09:10 PM #25
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
First off, I have to say up front that I have no experience with low SHBG and I've not done a lot of research into the literature. This is because I have the opposite problem of producing way too much SHBG and most of my research and experimentation has been with finding ways to deal with it being high. Originally Posted by BuzzardMarinePumper
I would not phrase it quite like you did, SHBG has nothing (that I know of) to do with receptor activity. What it does do is bind sex hormones and it has a particularly high affinity for androgens (like T and DHT). So this means with high SHBG, less of the androgens are available to bind to the receptors to stimulate the receptors to do their thing. Also, SHBG bound T will not pass through the blood-brain barrier, so while you may have sufficient Total T in the blood, your brain is starved of the hormone because SHBG won't let it through.
With low SHBG, more of the androgens (T, DHT, or whatever synthetic androgens you are taking) is available to bind and stimulate receptors. However, while higher free T/androgens is good, it also means that it will be metabolized by the liver and excreted much faster. That is why guys with low SHBG end up taking higher does of androgens to get the same effect, because they don't have sufficient SHBG to protect the androgens from liver metabolism. In this respect SHBG serves as a buffer for the androgens.
Bottom line is that both high and low SHBG is not a good thing but for different reasons. The bad news is that low SHBG is more difficult to treat. With high SHBG, you simply have to increase the dose so that you saturate the protein and enough of it spills over to the free form of the androgen to make you feel normal again (or build muscle if that's your goal). Also, as Kel mentioned, certain higher androgens in general suppress SHBG production and certain synthetic androgens will greatly suppress it, even at very low doses (e.g., Winstrol and Anavar ). I do not know if nandrolone has this same effect.
With low SHBG, there's not a lot you can do (that I know of) to beef up production of the protein. I've read of some guys having success with more frequent daily injections rather than weekly or even twice weekly injections. This will help to keep some active T in your body at all times and avoid the roller coaster of big injections and rapid metabolism by the liver.
-
05-13-2020, 08:07 AM #26
Knowledge Member on Prostate Cancer
- Join Date
- Oct 2012
- Location
- N. GA. Jaw Ja N A Cave
- Posts
- 1,946
- Blog Entries
- 1
Thank you ! Originally Posted by Youthful55guy
Yes I am sure I stated it incorrectly about receptors but in my old brain what stood out from past reads was lower SHGB is good because in some manner you get more bang for your buck with lower SHGB ........ Thank you for correcting me .
Could I possibly persuade you to try to dumb it down a little . I have had sever low SHGB to the point that it effects my Hematocrit (I think I mispelled this) numbers also = risk of heart failure and higher mortality rate ..... That is why I am so curious ...... My Dr is clueless ! So please anyone try to dumb it down and assist me in trying to understand . I have googled and low SHGB seems to be a somewhat unusual problem to treat - not that common ?
THank You Again !Last edited by BuzzardMarinePumper; 05-13-2020 at 08:09 AM.
-
05-13-2020, 01:51 PM #27
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Youthful55guy
It does and quickly. Matter of days is all it takes.-*- NO SOURCE CHECKS -*-
-
05-14-2020, 08:14 AM #28
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
I'll try. It is a somewhat complicated subject. Originally Posted by BuzzardMarinePumper
Guys who have low SHBG burn through T much faster than guys with normal or high SHBG. For a couple days after the injection, their Free T skyrockets and that drives Red blood cell (RBC) production. Hemoglobin and hematocrit are 2 ways to measure RBC production. Both T and DHT (to a grater extent) will push up your RBC production, so the more free T that is available, the more RBCs you produce.
The problem is that you burn through T so quickly, that with standard doses (e.g., 100mg in once weekly injections), you do not have a sufficient amount of T left in you system at the end of the week, so you feel like crap. To compensate (if you stick with once weekly injections), you inject larger and lager amounts of T so that you have something left at the end of the week to feel somewhat normal. However, this pushes your post-injection spike in blood T levels higher and high, and this drives RBC production faster and faster. Sometimes to dangerous levels.
Again, I have the opposite problem with SHBG, so I can only go off of what I've heard other guys discuss in various forums. The consensus among these guys is that when you have low SHBG, you are better off with more frequent injections of T rather than increasing the dose. So, for example, instead of bumping the weekly dose up to 200mg, you might consider injecting 20mg per day which equates to 140mg/week. This will help keep your Free T levels in the normal range throughout the week without driving huge spikes in Free T as you would with a larger 200mg once weekly dose. This will slow down RBC product to a more normal rate.
-
05-14-2020, 09:14 AM #29
 Knowledgeable Member
Knowledgeable Member
- Join Date
- Aug 2017
- Posts
- 2,368
As someone with chronically low shbg, Ive definitely found this to be the case. My results (and issues with side effects) are drastically improved with increased dose frequency. Originally Posted by Youthful55guy
Even with long ester cycles (Enanthate and Decanoate), Im better off with 4x/week pins. With short esters (acetate and prop), daily is pretty much mandatory, and Im sure that 2x/day would work even better, if I could be fucked to do it so often.
-
05-14-2020, 10:39 AM #30
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Give me an idea what your "low" actually is is you don't mind. Originally Posted by Gallowmere
What side effects did you have Gallo?-*- NO SOURCE CHECKS -*-
-
05-14-2020, 11:30 AM #31
Knowledgeable Member
- Join Date
- Aug 2017
- Posts
- 2,368
Tends to hover between 14-18 nmol, though admittedly its been about a year since I bothered having it checked. Originally Posted by kelkel
By side effects, I mean the usual stuff that comes with the various anabolics. More acne and subq water retention with test (even though my E2 is usually on the lower end, as I dont aromatize much). Similar with nandrolone , and the subq retention is pretty obvious with dbol even with its short halflife if I dont dose split. Masteron I didnt see any sides, but by the time I was stacking it, I was using MastE at 4x/week with the testE and deca .
Havent gotten around to trying Tren yet, but I wont be trying eod with ace anyway, as I already have a pretty good idea that Ill be much better off with ed.
-
05-14-2020, 02:01 PM #32
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Gallowmere
My last BW had my shbg at 8.1 on a scale of 19.3-76.4. To show what that does with testosterone , my total on 50mgs x 2 was 535 (LC/MS methodology) and my free was 39.9 on a scale of 6.6 - 18.1. Fascinating. Pulling more basic BW on Monday but not bothering with shbg....-*- NO SOURCE CHECKS -*-
-
05-14-2020, 02:29 PM #33
Knowledgeable Member
- Join Date
- Aug 2017
- Posts
- 2,368
Yeah, I had a similar thing with my free. It made my doctor freak out for a bit, so my next bw I left the free off, and he was fine with the total. Originally Posted by kelkel
The slavishness to ranges is goofy.
-
05-14-2020, 06:36 PM #34
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Gallowmere
Oh it's horrible how some doc's are that way. I could not imagine having to deal with docs like that. I'm fortunate to have a great relationship with my Uro. So much so that I just wrote up my script for Mondays BW a couple minutes ago.-*- NO SOURCE CHECKS -*-
-
05-14-2020, 07:05 PM #35
Associate Member
- Join Date
- Jan 2018
- Posts
- 172
From another forum: Originally Posted by Youthful55guy
"It's a misconception to think that low SHBG causes testosterone to be used up more quickly when on TRT. The rate of use is essentially controlled by the rate of absorption. One way to think of it is that the testosterone injections control the level of free testosterone, and the combination of free testosterone and SHBG determines where total testosterone ends up.
If conventional wisdom is correctabout more frequent injections being better for low-SHBG guysthen the likely reduction of peak estradiol may well be one of the reasons why. The idea is somewhat supported in theory by the decrease in the ratio of free testosterone to free estradiol as SHBG goes lower.
To clarify further, as I have in other posts, if you take a guy on TRT and lower his SHBG without changing other independent variables, then free testosterone must be basically unchanged, so total testosterone adjusts to match. This means that lower SHBG results in proportionally lower total testosterone. So from an absolute perspective, the variance in peaks and troughs is reduced, but as a proportion of average levels the variance is unchanged."
-
05-15-2020, 09:45 AM #36
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
What can I say? The individual that post it obviously has an opinion different then mine but has not data to back up the statements that are being made. Nor do I for that matter. I know of little (no) research for guys with low SHBG. I can only go off of the experience I've read from posts of guys dealing with the problem. Who's advice do you follow given that that there's no real data? I would say, develop your own data along with labs, and post them so that we can all benefit from the experience. That's what this forum is all about....exchange of information. Originally Posted by Ephemeral
-
05-15-2020, 10:33 AM #37
HRT Specialist ~ AR-Platinum Elite-Hall of Famer ~ No Source Checks
- Join Date
- Sep 2010
- Location
- East Coast Dungeon
- Posts
- 30,122
Originally Posted by Ephemeral
I've never seen this correlation and I've reviewed tons of bloodwork. It definitly does not relate to my BW.
Interesting though.-*- NO SOURCE CHECKS -*-
-
05-15-2020, 11:45 AM #38
Associate Member
- Join Date
- Jan 2018
- Posts
- 172
Can't type a lot now, my hand is injured. Originally Posted by kelkel
https://care.diabetesjournals.org/content/27/4/861
"221 middle-aged nondiabetic men
SHBG correlated well with total testosterone (r = 0.63, P < 0.0001), consistent with the biological role of SHBG as the major sex hormone-binding protein. This is in strong contrast to the lack of significant correlations between SHBG concentration and bioavailable and free testosterone (r = 0.07 and 0.1, respectively)."
-
05-15-2020, 12:48 PM #39
Senior Member
- Join Date
- May 2016
- Posts
- 1,218
This actually makes sense. As SHBG increases, it binds and protects SHBG from liver metabolism (as the theory goes). So, more SHBG means that you have more Total T because more of it is being protected. This has been my experience with high SHBG. Before TRT, I had moderately high Total T for a guy my age at the time (Total T = 680 ng/dL at age 55 with a normal range of 348-916). HOWEVER, my Free T was only 7.1 pg/mL (normal range 6.6-18.1). This is because the majority of my T production was being sucked up by SHBG and pushing up Total T because it was being protected from metabolism. Originally Posted by Ephemeral
So it makes perfect sense that there is a strong positive correlation between SHBG and Total T and no correlation between SHBG and Free T because at the high end of the SHBG curve, the amount of peripheral Free T is pretty much nonexistent.
-
05-16-2020, 01:33 PM #40
Knowledge Member on Prostate Cancer
- Join Date
- Oct 2012
- Location
- N. GA. Jaw Ja N A Cave
- Posts
- 1,946
- Blog Entries
- 1
Gentlemen I have my BW from Jan and can post it ......... Looks like crap but it has my Free T , Total T and SHGB on it + a lot of other stuff and it would be somewhat recent BW to view and compare your different thoughts ...... My MD that writes the script for my Test and Ai is a DA and I am fortunate to have this forum to read and make true decisions from ....
I posted a question about 6mths ago about low SHGB with little to not much response and no one really had info that seemed jermain ?
If you gents would care to view for my benefit and for you to compare to your thoughts I would be humbly grateful to yall

 Reply With Quote
Reply With Quote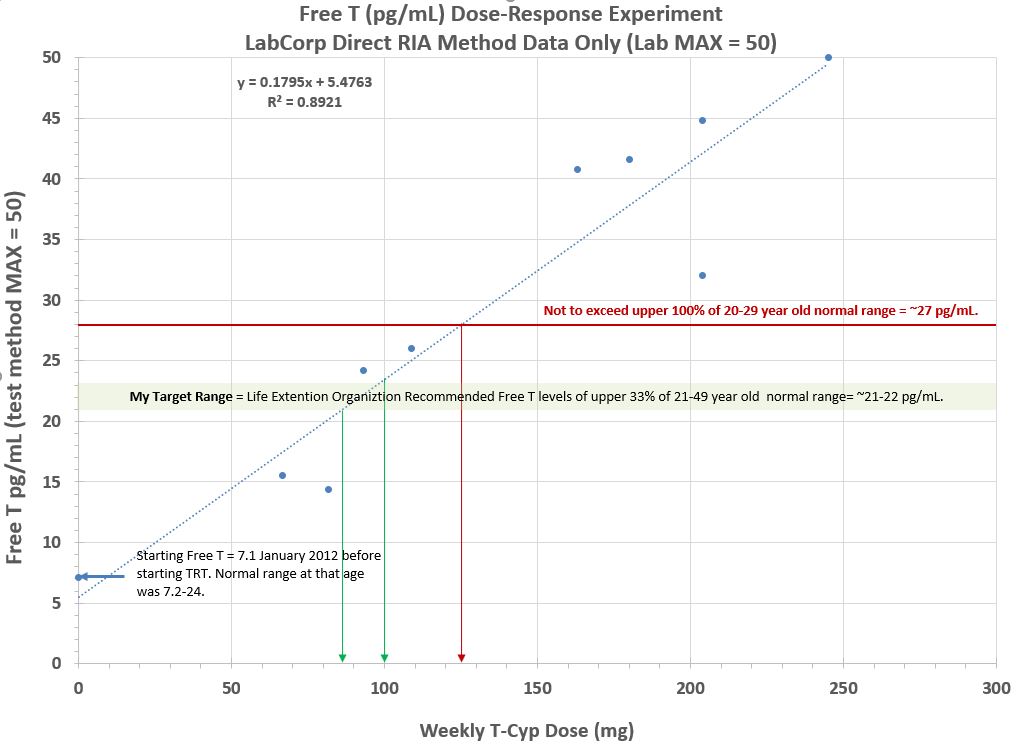
Thread Information
Users Browsing this Thread
There are currently 1 users browsing this thread. (0 members and 1 guests)






First Tren Cycle (blast)
Today, 11:29 AM in ANABOLIC STEROIDS - QUESTIONS & ANSWERS